KNEE INJECTION TECHNIQUES AND INDICATIONS
Injecting the knee is an important part of general practice, rheumatology and sports medicine. The technique and the indications are discussed below. Its application not only helps confirm certain diagnosis but also treat some conditions. This handout discusses the most common reasons for injecting and will, hopefully, make you more confident in this field.
Local anaesthetic is useful to make certain diagnoses. It can be used alone or mixed with corticosteroid. Short acting agents include Lignocaine, whilst longer acting agents include; Naropin, and Marcaine. There are certain toxic doses but these are unlikely to be exceeded in general practice. If in doubt consult the product information sheet.
You can use adrenaline but always avoid it’s use on extremities (i.e. digits) as it can cause vasoconstriction and gangrene.
Remember if you stick a needle into something you might think is infected send a specimen away.
Corticosteroid injections are used to relieve symptoms of arthritis in certain joints and are also used to reduce soft tissue inflammation. The appropriate use and knowledge of where and when to inject is extremely important.
INDICATIONS FOR LOCAL ANAESTHETIC ALONE
- Suturing a wound
- Diagnosis of pain coming from a certain part of the knee (e.g. bursa, iliotibial band). This is not common and usually should be done by a surgeon or sports physician.
WHAT ARE CORTISTEROIDS?
Corticosteroids are an anti-inflammatory medication which can be injected directly into a joint or around tendons. Corticosteroid is usually mixed with local anaesthetic to reduce pain which is usually only quite mild.
WHEN IS IT USED?
There are multiple indications and, discussed below are the common ones. In general, it is used to relieve inflammation of tendons or joints.
INTRAARTICULAR INJECTION
Intra-articular corticosteroids are primarily used for pain which is secondary to osteoarthritis. They can also be used in inflammatory conditions such as rheumatoid arthritis. They do not slow down or change the progression of arthritis.
- They are generally used in patients with arthritic symptoms who are not symptomatic enough to warrant a total joint replacement.
- It is also used when trying to delay an inevitable joint replacement.
- They are also useful in patients who are not medically fit for surgery
HOW LONG DOES IT LAST?
The effects usually take 24 – 48 hours to work. For the first day or two there can actually be a slight increase in pain as the corticosteroid starts to work. The effects can last anywhere from a week to 6 months, but it is only temporary. You can repeat the injections if required (up to three a year).
WHERE IS IT DONE?
Corticosteroids can be injected into the knee in the office under aseptic conditions.
CONTRAINDICATIONS
- Suspected infection in the joint
- Cellulitis
- Immunosuppression
- Allergy to local anaesthetic or steroids
- Joint replacement
SIDE EFFECTS
All side effects are low
- Risk of infection is very low (1 in 5000)
- Skin discoloration
- Fat necrosis
- Flare up of symptoms for a day or two
- Rise in sugar levels in diabetics- there is need to monitor levels carefully for two days
TECHNIQUE
The choice of steroid varies. Celestone is one of the more common steroids used:
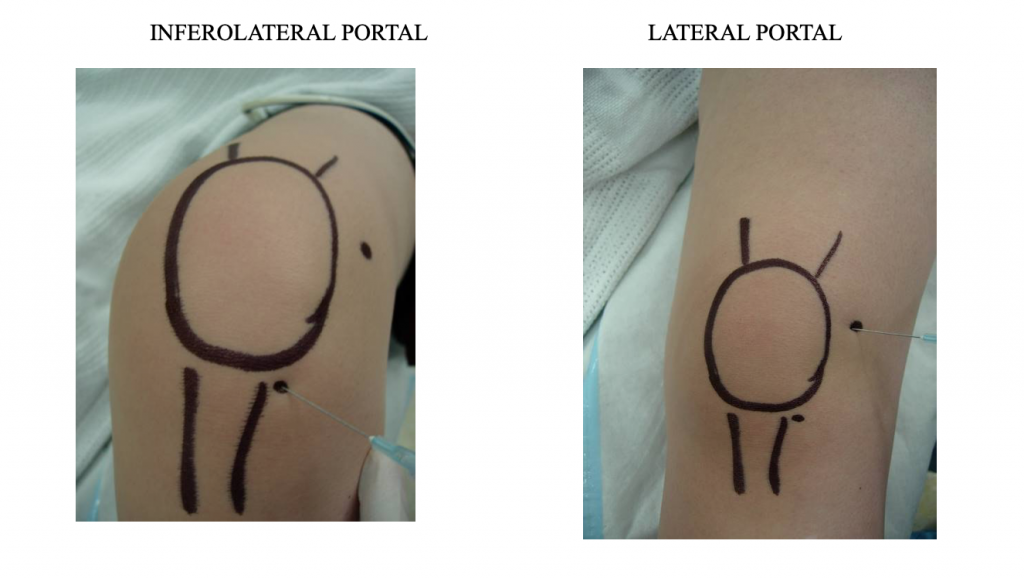
Mix 2 ampoules of Celestone with 3 mls of local anaesthetic (Lignocaine) in a 5ml syringe. Mix using an aseptic technique and use a blue or green (21G, 23G) needle. The choice of injection portal is either superolateral under the patella with the knee extended or through the inferomedial or inferolateral soft part of the knee with the knee flexed to 90 degrees. Always use an aseptic technique.
You do not need to aspirate the knee first unless there is a large effusion. If you do aspirate, send the fluid off for culture.
Other parts of the knee, may need to be aspirated or injected (e.g. the prepatellar bursa). This is superficial to the patella and can be traumatic or infective. If infective, aspirate heading straight down toward the patella, not into the knee joint. You should not be able to go into the joint because you will hit bone first.
Other bursa or fluid collections do occur. Aspiration or injection should only be done if you are sure of the diagnosis, otherwise you should seek an orthopaedic opinion. A Bakers cyst is extremely common and as a general rule should not be aspirated.