Knee Anatomy
The knee joint consists of the femur, tibia and patella. The femur (thighbone) is the bone connecting the hip to the knee. The tibia (shinbone) connects the knee to the ankle. The patella (kneecap) is the small bone in front of the knee. The fibula is a shorter and thinner bone running parallel to the tibia on its outside. The joint acts like a hinge but with some rotation.
The knee is connected by strong ligaments and surrounded by muscles. The muscles at the front of the thigh used to straighten the knee are the quadriceps and at the back to bend the knee are the hamstrings. The quadriceps tendon inserts into the patella at the top and the patella tendon comes off the bottom of the patella to attach to the tibia.
The ligaments of the knee joint stabilise the knee allowing it to function normally. The cruciate ligaments (anterior and posterior) are important structures, which guide the knee in its normal motion. Without these the knee often does not function normally and can result in instability or arthritis.
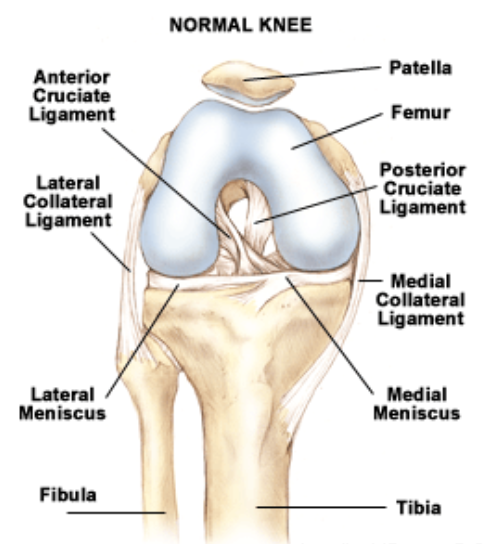 The medial ligament is on the inner side of the knee running from the femur to the tibia. The lateral ligament is on the opposite side of the knee running from the femur to fibula. These ligaments prevent sideways movement of the knee.
The medial ligament is on the inner side of the knee running from the femur to the tibia. The lateral ligament is on the opposite side of the knee running from the femur to fibula. These ligaments prevent sideways movement of the knee.
The knee is a synovial joint, which means it is lined by synovium, which produces fluid lubricating and nourishing the inside of the joint.
Articular cartilage is the smooth surfaces at the end of the femur and tibia. It is the damage to this surface which causes arthritis.
The meniscus is a specialised structure within the knee joint between the femur and tibia. There is a medial and lateral meniscus. These help distribute load, absorb shock, stabilise the knee and aid in lubrication.
Knee Arthritis
The knee joint is lined by articular cartilage, a specialised lining which allows smooth, painfree motion of the joint. Arthritis is a degeneration or wearing out of this lining which results in the bone ends rubbing on one another rather than the articular cartilage causing pain.
Types of Arthritis
Osteoarthritis: This form of arthritis can be due to normal ageing, or may develop as a result of another condition, past surgery or trauma. Heavy manual labour, obesity and a family history can predispose patients to osteoarthritis. The pain tends to be worse in the mornings and with vigorous activity.
Inflammatory Arthritis: The most common form is rheumatoid arthritis, an immune disorder resulting in inflammation of the synovial lining of the joint which releases chemicals and can subsequently damage the articular surface. This condition can affect any synovial joint in the body and is best treated medically by a rheumatologist. Knee replacement is only required when there is severe damage to the joint.
What are the symptoms?
- Pain – Usually of gradual onset but can be sudden. May be localised to one area in the joint or be all around the knee.
- Stiffness – It may be difficult to straighten or bend the knee
- Trouble walking – You may have a limp, grinding or clicking, or your joint may ‘give way’. These symptoms may be associated with limitation of walking due to either pain or fatigue
- Swelling – The inflammation might also make the joint feel hot and red.
- Deformity – The leg can change shape (become more bow legged or knock kneed)
How is it diagnosed?
Osteoarthritis is diagnosed on history, physical examination and X-ray. Physical examination will reveal pain on moving the joint and limitation of movement as well as osteophytes. X-rays will reveal narrowing of the joint space and often deformity of the bones and osteophytes. Blood tests are useful in inflammatory arthritis.
Non-operative treatment
Medical:
- Simple analgesia
- Anti-inflammatories supervised by local doctor
- Special medications for inflammatory arthritis
- Corticosteroid injections
- Weight loss
- Maintenance of fitness and muscle tone
- Use of a walking stick in the opposite hand to take weight off the knee
- Shoe inserts to absorb shock
- Glucosamine and chondroitin sulfate
- Hyaluronic acid injections
Operative treatment
Arthroscopy
This is a minimally invasive surgical procedure in which a miniature telescope-like instrument is passed into the joint so that the surgeon can see the inside of the knee in great detail, and operate through just two small incisions. This can help in early arthritis especially with sudden onset of symptoms. Often there is an associated meniscal tear, or loose flaps of cartilage which can be removed. An arthroscopy is useful in a knee that is not bad enough to warrant a replacement.
Osteotomy
This is an operation to cut the bone and realign it so that more weight is taken on the healthy part of the joint. It is particularly helpful in young active patients who are not suitable for a joint replacement.
Cartilage transplant
This is indicated in well-localised lesions in young patients.
Joint Replacement
This can be either a partial or a full knee replacement depending on symptoms and X-ray signs.