Total Hip Replacement
Total Hip Replacement Video
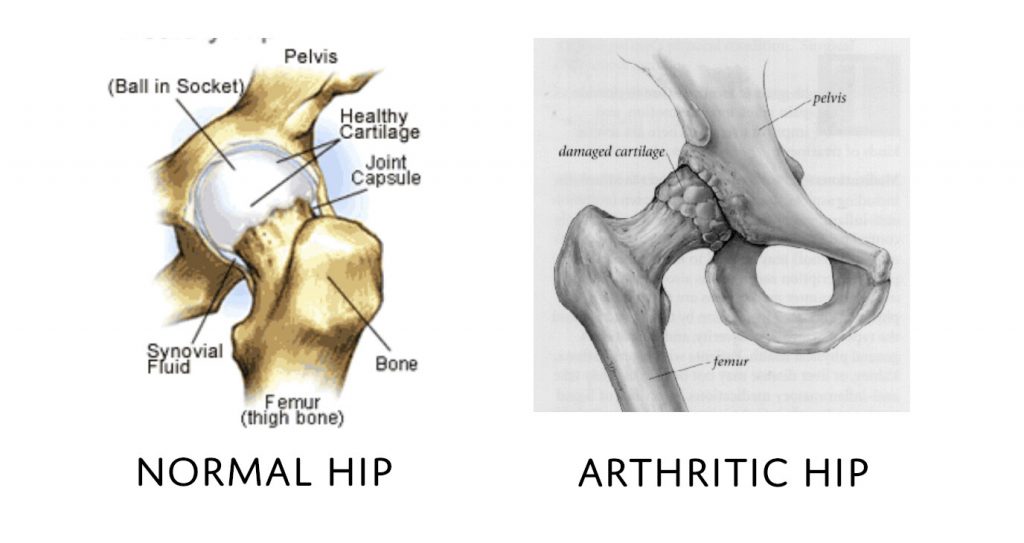
Hip Anatomy
The hip joint is composed of a ball and socket joint. The femoral head (ball) is the top of the femur (thigh bone) and the acetabulum (part of the pelvis) is the socket. These surfaces are both covered by articular cartilage, which is a specialised lining allowing smooth pain free motion of the joint. Damage to this lining is called arthritis.
Inflammation of the synovium surrounding the joint is called inflammatory arthritis; the most common of which is rheumatoid arthritis.
The labrum is a specialised structure going around the rim or edge of the acetabulum adding to stability of the joint. Damage to this structure can result in catching causing pain in the joint.
There are also several strong ligaments holding the hip joint in place. Around the joint are muscles which move the hip and allow us to move.
Introduction
What causes a painful hip?
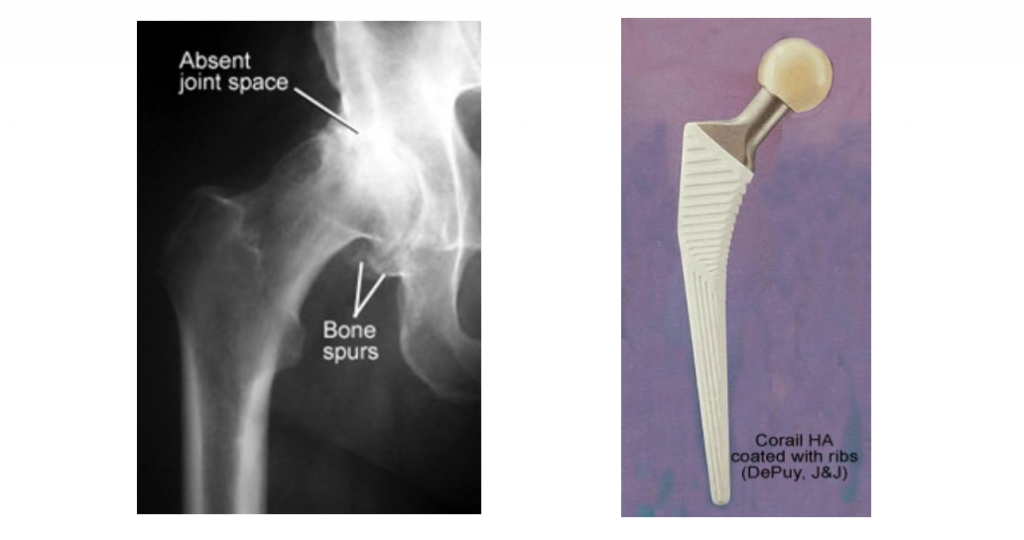
When one or more parts of the hip are damaged, it can become painful and movement becomes restricted. Over time, cartilage (the smooth covering at the ends of the bone in the joint) starts to crack or wear away. When this happens, the bones making up the joint rub together. This is arthritis. Its severity varies from mild to severe.
Any of the problems below may lead to joint damage and hence hip pain:
OSTEOARTHRITIS
As you get older the hip can wear out through overuse, trauma, childhood issues etc. Unfortunately, there is no way to stop this progressing and there is no way to reverse it.
INFLAMMATORY ARTHRITIS
This is a group of conditions where the lining of the joint becomes inflamed and secretes material that destroys the joint cartilage. Due to the nature of these conditions, more than one joint is usually affected. The joints are hot, swollen and painful and deformity is common. An example of this is rheumatoid arthritis.
AVASCULAR NECROSIS
This is where the femoral head collapses. This can occur for no reason (idiopathic), following a bad injury (fracture) or can be secondary to a number of conditions (e.g. long-term use of alcohol or steroids). It is due to loss of blood supply to the bone. If the bone dies (necrosis), the joint will become arthritic. This pain often comes on quite suddenly and tends to increase rapidly. This can happen at any age but is particularly common in young adults.
FRACTURE
A bad fall or injury to the hip can break (fracture) the bone. A fracture can also lead to avascular necrosis.
CHILDHOOD HIP PROBLEMS
Occasionally hip pain results from a problem which had started in childhood. Such conditions include a poorly formed hip joint (dysplasia or congenital dislocation of the hip), an infection (of the hip joint), problems with blood supply to the hip (Perthes disease) or trauma.
INFECTION
Infection can destroy the cartilage lining leading to osteoarthritis.
OTHER CAUSES
A bad injury that did not heal properly
A chronic illness (e.g. kidney failure)
Obesity
Other rare diseases affecting bones or soft tissue
What is a hip replacement?
Total hip replacement is a “quality of life” elective operation, offered to patients when their pain and disability are significant as a procedure that will decrease their discomfort.
Total hip replacement, although dating back to the 1940’s, was advanced by British in the 1960’s. Since then it has become a very common procedure with continual advances being made.
The hip is opened up through various techniques, none of which is definitely better than the other. All have their advantages and disadvantages.
The arthritis is cut out by cutting across the femoral neck.
The femur and acetabulum are then prepared for what are called trial components and the hip checked for stability and leg length. The real components are then inserted. These consist of a femoral component that goes into the femur. This is either uncemented or cemented. On top of the femoral component is placed the round ball, or femoral head, made of metal or ceramic.
The acetabular component is similarly inserted. This is generally uncemented. Inside this goes a liner, generally a high-density polyethylene.
The hip is then reduced and the soft tissues closed.
There are many different types of prosthesis. Dr Walker will choose what he believes is the best one for your requirements.
Benefits
Hip replacement surgery is one of the best operations available to surgeons. It is an extremely successful operation in the right hands for the right reason. During this surgery your problem hip joint is replaced with an artificial joint (a prosthesis). After a total hip replacement, you can look forward to moving more easily and without pain.
Most people gain all of the following benefits:
- Stops or greatly reduces hip pain. Even the pain from surgery should go away within weeks
- Increases leg strength. Without hip pain you will be able to use your legs more and build up your muscles
- Improves quality of life by allowing you to do activities of daily living and low impact activities in greater comfort
- Enables you to sleep without pain
- Provides years of reliable function. Most total hip replacements last for many years. The revision rate is roughly 0.5% per year.
When should you have a hip replacement?
Surgery should be considered when you have arthritis on your x-ray, in conjunction with pain and stiffness from your hip joint causing:
- Severe disability
- Inability or difficulty to perform your job
- Interference with your leisure activities or walking/ mobility
- Difficulty putting on your shoes and socks
- Sleep disruption
- When conservative treatment such as analgesia, anti-inflammatories, weight loss, physiotherapy and aids like crutches or a cane has failed
Remember, it is an elective procedure and should only be performed when you are no longer prepared to put up with your pain and disability. It is important to understand the benefits versus the risks involved.
Pre-Operation
Pre-Admission Clinic
You will usually be required to attend a preadmission clinic and/or see a physician prior to your surgery and have some simple tests. The tests required are:
- Blood tests to ensure your blood count is normal and you have no other major medical problems.
- ECG, wherein a Cardiograph of your heart will be taken to make sure you have no underlying cardiac problems.
- X-rays. Always bring x-rays of your hip to hospital. Dr Walker may or may not require new x-rays of the hip he is operating on.
- Urine sample to ensure you do not have a urinary tract infection. An infection anywhere before surgery e.g. infected toenail, skin lesion, throat infection, gum or dental infection can greatly increase your chances of infection of the joint replacement following surgery. If an infection is found, it will be treated with simple antibiotics prior to surgery.
All relevant information about what to do before, during and after your stay in hospital will be discussed at length at this clinic.
Medications
- 10 days prior to surgery, cease aspirin and anti-inflammatory medications (e.g. Voltaren, Feldene) as they may cause bleeding.
- 10 days prior to surgery cease any naturopathic or herbal medications as these may also cause bleeding.
- Continue with all other medications unless otherwise specified.
Home Preparation
- Arrange for someone to help out with everyday tasks like cooking, shopping and laundry
- Put items that you use often within easy reach before surgery so you won’t have to reach and bend as often
- Remove all loose carpets and tape down electrical cords to avoid falls. Make sure you have a stable chair with a firm seat cushion, a firm back and two arms
- Make sure your shower or bath is safe and easy to get in and out of. Handrails, non-slip mats and suitable stools to sit on are helpful for personal safety and comfort
Other
- Notify Dr Walker if you have any abrasions, cuts or pimples around the hip.
- Bring any X-rays, MRI scans or other relevant investigations you have had done to your surgery.
- You are advised to stop smoking for as long as possible prior to surgery.
Procedure
- The anaesthetist will see you before the surgery. They will discuss with you if they are going to do a spinal or general anaesthetic.
- You are taken to the operating theatre and while you are still awake, you are placed on the operating table and set up for surgery.
- A urinary catheter will be placed in your bladder to measure your fluid balance during and after surgery.
- A cut is made in the skin and underlying tissues to expose the hip.
- The hip joint is dislocated and the head sawn off.
- Special instruments are used to make very accurate cuts in the bone to fit the prosthesis.
- Trial components are put in first to make sure everything fits properly.
- The bone is then cleaned to remove debris.
- The real components are then inserted with or without cement.
- Drains are usually inserted.
- The wound is then carefully closed in layers, the last being the skin.
- A dressing is applied and you are taken to recovery.
Post-Operation
After Your Operation
- Your hip will be heavily dressed with large pads and sticky dressings.
- You may have a large triangular shaped pillow placed between your legs.
- Your fluid input and output are measured carefully. A drip in the arm will be used to give you fluid, replace blood during the operation and for antibiotics.
- Pain is normal after the operation but if your pain is not reduced be sure to tell the nurse. Pain medication may be injected into a muscle or delivered by IV into the blood stream.
- The drip, drains and catheter are removed approximately 24 hours after surgery.
- Blood will be taken 24 to 48 hours after the operation to check your haemoglobin and electrolytes.
- Your exercise regime will begin as soon as you are capable and this will continue during your stay in hospital and once you are at home. Often you will be walking on the day of surgery. A physiotherapist will supervise this.
- You will be discharged 3 – 5 days post-operatively depending on your progress. In some cases, you will be sent to a rehabilitation centre before you go home to have some hydrotherapy and physiotherapy.
- Sutures are either dissolvable or staples. Staples are removed at about 12 days post-surgery and require a special staple remover.
Recovery
- You are in hospital approximately 3 – 5 days. At Day 1 or 2 you will get up on a frame and then you progress to crutches and then a stick usually by 4 – 6 weeks.
- You usually go from hospital to rehabilitation and are in rehabilitation for 1 – 2 weeks. This will include aggressive physiotherapy and hydrotherapy.
- When you leave hospital, you will probably still require pain relief tablets but no injections. Wean your medications down to Panadol as soon as possible.
- It is best to avoid anti-inflammatories if you have arthritis elsewhere for 1 week to avoid any possible bleeding.
- You should sleep with a pillow between your legs for 6 weeks to avoid possible dislocation.
- Driving is typically allowed at 6 weeks.
- By 12 weeks you can usually walk as far as you want to.
- People usually can return to work somewhere from 6 – 12 weeks. Heavy manual work may take longer. Normally by 3 months you can play sports like golf, bowls, stationary bike ride, bush walk, doubles tennis and swim.
- Driving typically allowed at 6 weeks.
Results
This operation is one of the most successful operations available today. It is an excellent procedure to improve a person’s quality of life. After this operation 98% of people are good or excellent. Good means, occasional aches and pains which do not require painkillers and excellent means no significant pain or discomfort. There are some people who will have unexplained pain.
In general, 90 –95% of hips survive 15 years but this depends on a number of variables such as your age and activity level. For a hip, we use the analogy of a tyre. The more you drive on it the quicker it wears out. The better it is looked after and serviced the longer it will last.
Special Precautions to Take
- Remember this is an artificial hip and must be treated with care.
- In general, the more active you are the quicker your hip will wear out.
- You can drive when you have regained muscle control, usually by 6 weeks.
- Avoid situations where you might fall.
- Your hip may make the alarm go off in a metal detector at the airport. You can receive a note from the doctor’s rooms to say you have had a joint replacement.
- Prevention of infection is vital. If you have any infections anywhere make sure you see your local doctor straight away for treatment. If you get increasing pain in your joint, are sick and have a temperature you should go to hospital to get checked out.
- To minimise the risk of dislocation, do not flex the hip beyond 90 degrees and internally rotate at the same time.
Antibiotics should be prescribed if you have an infection anywhere in the body, if you have surgery in contaminated areas such as teeth, nose, bowel or bladder, podiatry treatment or urinary catheterisation.
Activities Post-Surgery
- You should avoid placing excess stress on the joint, this may occur through ‘pounding activities.
- Walking is good.
- Swimming in a pool or light surf between the flags is safe.
- Doubles tennis is allowable but anything more aggressive will lead to premature wear of your joint.
- Contact sports are prohibited and jogging can be detrimental to the long-term survival of your joint replacement
- Skiing on groomed slopes if you are a good skier is acceptable as long as you are aware you can cause significant damage if you fall.
- Bowls and golf should not be a problem after your hip replacement.
Risks and Complications
Any operation, big or small, has risks. The following can occur with any surgery and some rarer complications may also be possible. The utmost care is taken at all times during surgery to prevent these complications. Dr Walker is a subspecialist and operates within his defined area of expertise. This minimises the risk of complications.
You will need to sign a consent form prior to your surgery stating that you understand these risks and wish to go ahead with the surgery. Complications can be related to the anaesthetic or general in nature.
Some complications specific to total hip replacement are:
- Infection
- Fracture of femur or pelvis
- Damage to nerves or blood vessels
- Blood clots (deep vein thrombosis or pulmonary embolism)
- Wound irritation or breakdown
- Trochanteric bursitis
- Dislocation
- Leg length inequality
- Wear
- Osteolysis
- Limp
- Heterotopic ossification
- Cosmetic appearance
- Breakage of the implant
The above list is not exhaustive. For more information on complications:
Total Hip Replacement Complications
Frequently Asked Questions
When can I go back to work?
People usually can return to work somewhere from eight to twelve weeks. Heavy manual work may take longer.
When will I be able to drive again?
When you feel comfortable and when you have regained muscle control. For most people, this is usually by six weeks. Please also check with your insurance company as they may have specific rules on when you can drive after surgery.
When will I be able to resume sexual intercourse?
Sexual intercourse is allowed when the patient is comfortable but they have to be in charge of the positions used and any significant discomfort should result in the patient abstaining until they talk to their doctor.
In general, sexual intercourse occurs at around three to six weeks post operatively.
When will I be able to do exercise again?
Normally by three months you can play sports like golf, bowls, stationary bike ride, bush walk, doubles tennis and swim. Jogging and heavy weights, although possible, will wear the joint prematurely. Contact sports are not appropriate.
Remember this is an artificial hip and must be treated with care.
In general, the more active you are, the quicker your hip will wear out.
Avoid situations where you might fall.