MENISCUS TEARS
FUNCTION
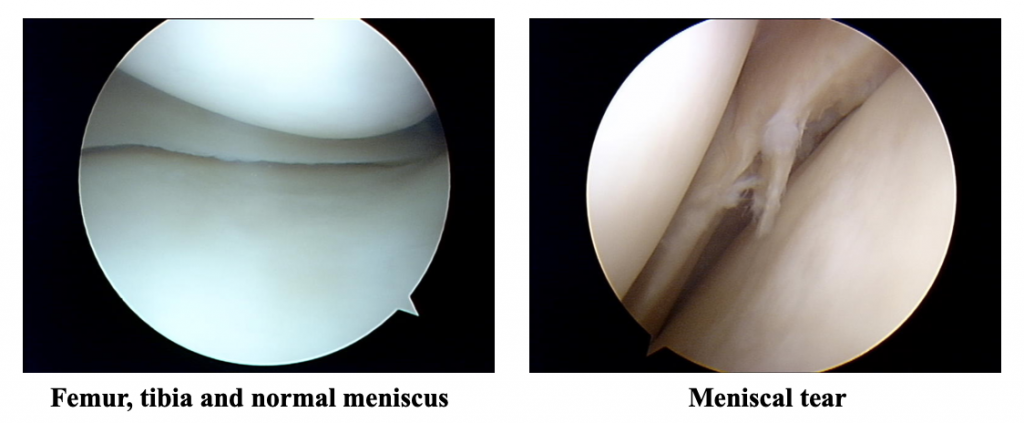
The meniscus is a soft rubbery structure between the femur and tibia. There is one on both sides of the knee (a medial and lateral). Meniscal tears are very common. The meniscus is often referred to as cartilage. Articular cartilage is the smooth lining of the joint at the ends of the bone.
The meniscus acts as a:
- Shock absorber to take some of the force within the knee
- Stabiliser of the knee
- Lubrication assistant
Once a meniscus is torn, it no longer functions as it should and if symptomatic is best partially removed. Once torn, due to the very poor blood supply to the meniscus, it is unlikely it will heal itself. Tears are described according to the type of tear as simple or complex. Without the meniscus there is an increased risk of osteoarthritis in the long term. The severity and timing of arthritis depends on numerous factors such as age, activity levels, weight and degree of meniscal damage. This is usually a very slow process.
HISTORY OF INJURY
There does not need to be a specific injury. Athletes usually but not always tear their meniscus with a specific injury (usually a twisting force) but in older people it can result from minimal or no trauma. Some people will feel a ‘pop’ or something ‘go’ in the knee. The pain is not usually severe and most people can continue with sports or at least can walk around without too much pain.
SYMPTOMS AND SIGNS
- Swelling
- Pain is usually localised to the side of the knee where the tear is
- Locking of the knee. When the knee gets stuck so you can’t move it. Usually it can’t be straightened. This is because a fragment of the meniscus gets stuck between the bones.
- Giving way usually caused by pain
- Clicking
DIAGNOSIS
This can usually be made on the history and examination. An MRI test may be ordered to confirm the diagnosis and to exclude other pathology. However, this is not always necessary and may delay treatment. MRIs vary in their quality and are not always correct.
TREATMENT
Initial treatment involves rest, ice, elevation and bandaging. There is no urgency to be seen by a surgeon unless you have a locked knee, in which case you risk damage to the meniscus as it gets caught between the bones of the knee joint.
If the pain does not resolve with conservative treatment, surgery may be warranted.
RESULTS
Arthroscopy is a small operation with a low risk of complications. The results depend largely on whether or not there is damage to other structures in the knee. If there is damage to the articular cartilage or smooth lining of the joint, the success of the procedure is reduced. The more arthritis you have, the less successful the procedure is and hence the indications are limited.
MENISCAL REPAIR
There is limited potential for the meniscus to heal, due to the poor blood supply. Only tears in the outer half of the meniscus have the potential to heal. The decision to attempt a repair is based on age, activity levels, occupation and sporting demands.
Most patients with a repairable meniscus are under 45 years old and up to 80% of these are associated with a tear of the anterior cruciate ligament. An MRI scan helps determine the extent of the tear but the final decision to repair can not be made until the time of surgery as it depends on the size, site and quality of the remaining meniscus. There is no point in repairing a meniscus which is unlikely to heal.
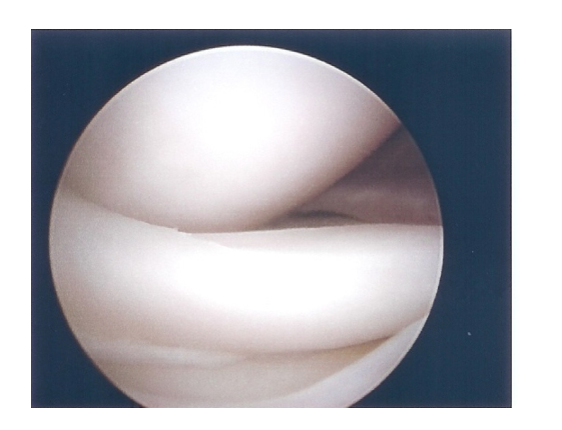
BUCKET HANDLE MENISCUS TEAR
Part of the meniscus flipped into the joint
Repair can usually be performed arthroscopically without any separate incisions using special devices, but occasionally one or two other incisions in the skin may be required.
There are advantages and disadvantages of meniscal suture:
ADVANTAGES
- Maintain protective role of meniscus
- Reduces the risk of arthritis
DISADVANTAGES
- Longer rehabilitation period
- Longer restriction of work and sport activities
- Failure of the meniscus to heal (15-20%) due to its poor blood supply
- Slightly increased risk to neurovascular structures
- Damage to articular surface from some of the devices used
Overall if a meniscus can be repaired (in the right patient with the right type of tear) it is best to do so as it protects the knee from premature arthritis.
POST-OP INSTRUCTIONS
The post-op instructions will vary from one knee to another depending on the extent of the repair and damage to other structures. Usually the surgery is done as a day only procedure. You may require crutches and/or a splint. Your weight bearing and bending may be restricted again depending on the extent of the repair. Time required off work varies from a few days to a few months depending on your occupation.
If your meniscus does not heal, you may develop ongoing symptoms and require further arthroscopic surgery to remove the torn portion of the meniscus which has not healed.